HIV Combo Test: Window Period, Results and What They Mean
Reviewed by the LabReadAI medical team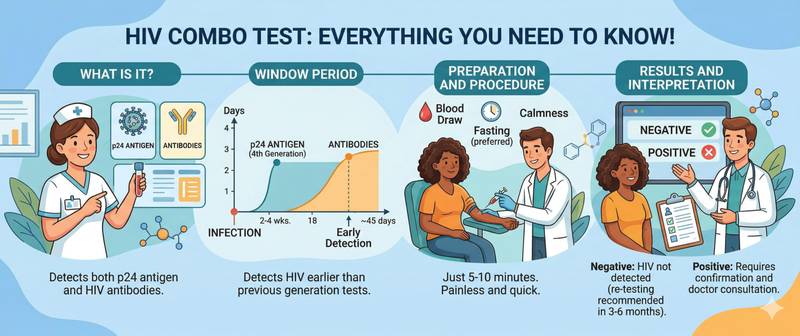
The HIV Combo test is a fourth-generation assay that simultaneously detects antibodies to HIV-1 and HIV-2 along with the p24 antigen of the virus. This dual detection principle makes it the most reliable screening tool available: the p24 antigen appears in the blood before antibodies form, narrowing the diagnostic window to just 2–6 weeks after infection. Understanding how this test works, when to take it, and how to read the result helps avoid unnecessary panic and ensures timely treatment.
What the HIV Combo Test Is and How It Differs from Earlier Generations
HIV testing has gone through four generations of evolution. Each successive generation shortened the seronegative window — the period between infection and the moment the test can detect it.
| Generation | What it detects | Diagnostic window | Current use |
|---|---|---|---|
| 1st generation | IgG antibodies to HIV-1 | 8–12 weeks | Obsolete |
| 2nd generation | IgG antibodies to HIV-1 and HIV-2 | 6–8 weeks | Rarely used |
| 3rd generation | IgM + IgG antibodies to HIV-1/2 | 4–6 weeks | Limited use |
| 4th generation (Combo) | IgM + IgG antibodies + p24 antigen | 2–6 weeks | Standard of care |
The p24 antigen is a viral capsid protein that enters the bloodstream as early as 11–14 days after infection — before the immune system mounts an antibody response. Once the body begins producing antibodies, free p24 levels decrease (it becomes bound in immune complexes), but by that point the test already detects antibodies. The HIV Combo thus covers both phases of the immune response.
The Seronegative Window: When the Test Cannot Yet Detect Infection
The seronegative window is the primary source of anxiety for people after a potential exposure. For a fourth-generation test, it averages 18–45 days but in rare cases may extend to 6 weeks.
Practical testing timeline recommendations:
- 2 weeks after exposure — the test can detect p24 antigen in some infected individuals (sensitivity approximately 60–70%)
- 4 weeks — sensitivity reaches 95%
- 6 weeks — a negative result virtually excludes infection (sensitivity > 99%)
- 12 weeks — follow-up test for definitive exclusion (WHO and CDC recommendation)
If post-exposure prophylaxis (PEP) was taken, the window may be extended — a follow-up test 12 weeks after completing the course is mandatory.
When You Should Get an HIV Combo Test
HIV testing is not only for suspected exposure. There are several clinical and preventive indications:
- Unprotected sexual contact with a partner of unknown status
- Blood exposure (needle stick, medical accident)
- Pregnancy planning and prenatal care
- Unexplained weight loss, prolonged fever, enlarged lymph nodes
- Recurrent infections suggesting compromised immunity
- Before elective surgical procedures
When immunity is compromised, a complete blood count frequently reveals lymphopenia. A drop in lymphocyte levels below the reference range may be the first laboratory sign of immunodeficiency and a reason to order HIV testing.
How to Prepare for the Test
The HIV Combo test does not require complex preparation, but following basic guidelines reduces the chance of technical errors:
- Fasting is not required — the test can be taken after eating
- Abstain from alcohol for 24 hours before the test
- Medications do not affect the result (except antiretroviral drugs and PEP)
- Physical activity and stress do not distort the result
- Blood is drawn from a vein into a standard collection tube
Results are typically available within 1–3 business days. Rapid fourth-generation point-of-care versions (from capillary blood) provide an answer in 15–30 minutes, but their sensitivity is somewhat lower than laboratory-based EIA.
Interpreting Results: Reactive and Non-Reactive
HIV Combo results are not reported as "positive" or "negative" — the terminology used is "reactive" and "non-reactive."
| Result | Meaning | Next steps |
|---|---|---|
| Non-reactive | No antibodies or p24 antigen detected | If window period has elapsed — HIV infection is excluded |
| Reactive | A reaction was detected (antibodies and/or antigen) | Confirmatory testing is mandatory |
| Indeterminate / grey zone | Borderline signal | Repeat test in 2–4 weeks |
Important: a reactive screening result is not a diagnosis. Every reactive HIV Combo result must undergo confirmation by a second method.
Confirmatory Testing: What Happens After a Reactive Result
The confirmation algorithm varies by national protocol, but the general principle is the same:
- Repeat EIA/CLIA — the test is repeated in duplicate from the same serum sample
- Immunoblot (Western blot) — detects antibodies to specific HIV proteins (gp120, gp41, p24, p31, etc.). It is considered confirmatory when antibodies to at least two proteins are identified
- HIV RNA PCR — direct detection of viral nucleic acid, used when the immunoblot is indeterminate or for early diagnosis
A definitive diagnosis is established only after all stages are completed. No single reactive EIA result constitutes grounds for an HIV diagnosis. More on the disease, its symptoms and transmission is in HIV and AIDS.
False-Positive and False-Negative Results
No laboratory test has absolute accuracy. The HIV Combo has a specificity of 99.5–99.8%, but in mass screening even 0.2% false reactivity produces a noticeable number of erroneous reactive results.
Causes of false-positive results:
- Autoimmune diseases (systemic lupus erythematosus, rheumatoid arthritis)
- Recent vaccination (influenza, hepatitis B)
- Pregnancy — cross-reactivity of maternal antibodies
- Multiple blood transfusions
- Laboratory technical errors
Causes of false-negative results:
- Blood drawn during the seronegative window
- Use of antiretroviral therapy or PEP
- Agammaglobulinemia and severe immunodeficiencies (extremely rare)
- HIV-2 infection when using assays with insufficient HIV-2 sensitivity
Changes in the leukocyte differential — leukopenia or neutropenia — can accompany HIV infection and serve as an additional indirect sign during result interpretation.
When to See a Doctor
- Reactive HIV Combo result — seek an infectious disease specialist immediately for confirmatory testing
- Non-reactive result but persistent symptoms (fever, weight loss, enlarged lymph nodes) — repeat testing in 4–6 weeks and expanded workup
- Exposure to an HIV-positive partner less than 72 hours ago — emergency consultation for post-exposure prophylaxis
- Planning pregnancy — both partners should be tested before conception
Early detection of HIV infection and timely initiation of antiretroviral therapy allow patients to achieve an undetectable viral load, preserve immune function, and maintain a near-normal life expectancy.
This article is for informational purposes only and does not replace professional medical advice. If you receive a reactive result, consult an infectious disease specialist for confirmatory testing.
For informational purposes only
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Please consult a healthcare professional for medical guidance.