Progesterone in Women: Normal Range by Cycle Day and Day 21
Reviewed by the LabReadAI medical team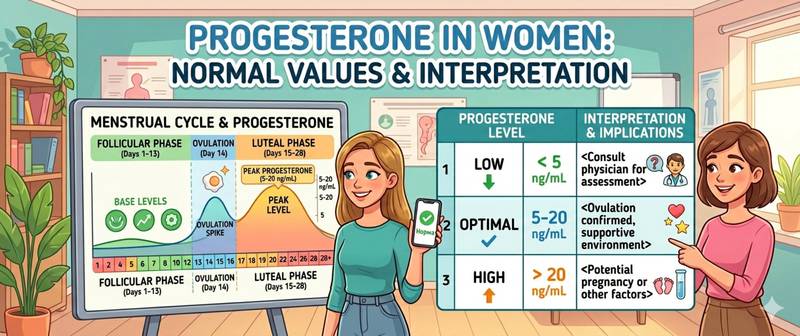
Progesterone is the second-phase menstrual cycle hormone, the principal regulator of reproduction, and at the same time a powerful neurosteroid with calming effects. The fall in progesterone before menstruation and in perimenopause is a frequent but underappreciated cause of anxiety, sleep disturbance, and emotional lability in women. Here's how to test progesterone correctly, what the norms are by cycle day, and why deficiency is so often missed.
What Progesterone Is and How It Works
Progesterone is a steroid hormone synthesized mainly by the corpus luteum of the ovary in the second half of the cycle, by the placenta during pregnancy, and in small amounts by the adrenal glands in men and non-pregnant women.
Its main functions:
- Endometrial preparation for implantation — without progesterone the embryo cannot attach to the uterine wall
- Pregnancy support — hence the name (from Latin pro-gestare, "for gestation")
- Estrogen antagonism — balances the proliferative effect of estradiol on tissues
- Neurosteroid effect — the metabolite allopregnanolone activates GABA-A receptors, acting as a natural tranquilizer
- Basal body temperature regulation — raises it 0.3–0.5 °C in the second cycle phase
- Sleep modulation — sedative effect through the GABAergic system
The link between progesterone and anxiety operates via allopregnanolone, which acts on the same GABA-A receptor as benzodiazepines. So a fall in progesterone (PMS, perimenopause, luteal insufficiency) produces a "benzodiazepine withdrawal" picture — anxiety, insomnia, emotional lability.
Progesterone is the biochemical partner of cortisol: both are synthesized from the shared precursor pregnenolone. Under chronic stress, cortisol "takes" pregnenolone away from progesterone — the "progesterone steal" phenomenon.
Normal Progesterone Range by Cycle Day
Progesterone levels change radically through the cycle. Without specifying the day, any value is misinterpreted.
| Period / phase | Normal (nmol/L) | Normal (ng/mL) |
|---|---|---|
| Follicular phase (days 1–14) | 0.3–2.2 | 0.1–0.7 |
| Ovulation (~day 14) | 0.5–9.4 | 0.2–3.0 |
| Luteal phase (days 15–28, peak on day 21) | 6.9–56.6 | 2.2–18.0 |
| First trimester pregnancy | 32.6–139.9 | 10.2–44.0 |
| Second trimester pregnancy | 62.0–262.4 | 19.5–82.5 |
| Third trimester pregnancy | 206.7–728.2 | 65.1–229.1 |
| Postmenopause | < 0.5 | < 0.2 |
Unit conversion: nmol/L × 0.3145 = ng/mL.
17-OH progesterone is a separate marker, not to be confused with the standard one. It is used to diagnose congenital adrenal hyperplasia, with norms:
| Period | 17-OH progesterone normal (nmol/L) |
|---|---|
| Follicular phase | < 2.4 |
| Luteal phase | 1.0–8.7 |
| Postmenopause | < 2.1 |
How to Test Progesterone Correctly
Critical: timing determines everything.
Standard schedule:
- Tested on day 21 of the cycle (in a standard 28-day cycle) — the peak of the luteal phase
- With irregular cycles — 5–7 days before the expected menstruation
- When monitoring ovulation — 7 days after presumed ovulation (by ultrasound or basal temperature)
- Fasting, in the morning (8:00–11:00 AM)
Preparation:
- 8–14 hours fast before the draw
- Avoid alcohol for 24 hours
- No smoking for 1 hour
- Disclose oral contraceptives, progesterone-containing medications (Utrogestan, Duphaston), and benzodiazepines
- For ovulation work — repeat in 2–3 days for accuracy
For luteal-phase and estrogen-progesterone balance assessment, progesterone is usually drawn alongside estradiol, FSH and LH — conveniently as a sex hormone panel.
Causes of Low Progesterone
Low luteal-phase progesterone is a frequent and often missed cause of infertility, PMS anxiety, and sleep disturbance.
Luteal insufficiency:
| Cause | Mechanism |
|---|---|
| Chronic stress | "Progesterone steal" toward cortisol |
| Hypothyroidism (TSH > 2.5) | Reduced corpus luteum function |
| Hyperprolactinemia | Prolactin suppresses progesterone synthesis |
| Polycystic ovary syndrome (PCOS) | Disrupted ovulation → no functional corpus luteum |
| Vitamin D deficiency | Impaired steroidogenesis |
| Low cholesterol (< 4.2) | Substrate deficiency for steroid synthesis |
| Strict diets, low body fat percentage | Hypothalamic suppression |
| Perimenopause | Reduced ovulation → luteal insufficiency |
Symptoms of progesterone deficiency:
- PMS anxiety, emotional lability in the second cycle phase
- Insomnia and awakenings 7–10 days before menstruation
- Painful, heavy menstruation
- Short luteal phase (< 12 days) or pre-menstrual spotting
- Breast tenderness, edema, premenstrual weight gain
- Infertility, recurrent pregnancy loss
- Estrogen dominance symptoms: fibroids, endometriosis, fibrocystic breast
Progesterone and Anxiety: The GABAergic Link
This is one of the most clinically important aspects. The progesterone metabolite allopregnanolone is a powerful GABA-A receptor modulator, working through the same mechanism as benzodiazepines. When progesterone falls before menstruation or in perimenopause, allopregnanolone falls too — and the nervous system loses its natural tranquilizer.
Clinically this presents as:
- PMS anxiety — heightened anxiety 7–10 days before menstruation
- Perimenopausal anxiety — progesterone fluctuations produce "waves" of anxiety
- Sleep disturbance cyclically tied to cycle phase
- Irritability, emotional lability, reduced stress tolerance
For the full picture, see anxiety: which lab tests to take. For chronic stress and "progesterone steal," see how to lower cortisol.
High Progesterone: Causes
Elevated progesterone is rarer than deficiency and most often physiological:
- Pregnancy (main cause — expected progesterone rise)
- Luteal cyst of the ovary
- Progesterone-containing medications (Utrogestan, Duphaston, progesterone IUDs)
- Congenital adrenal hyperplasia (elevated 17-OH progesterone)
- Choriocarcinoma, hydatidiform mole (significant elevation)
- Adrenal or ovarian tumors (rare)
An isolated moderate luteal-phase elevation in a non-pregnant woman is usually a normal variant.
When to See a Doctor
Endocrinology or reproductive endocrinology consultation is indicated for:
- Confirmed luteal insufficiency (low day-21 progesterone in two cycles)
- Infertility and recurrent pregnancy loss
- Severe PMS with depressive-anxious symptoms
- Cycle disruption lasting more than 3 months
- Suspected non-classical CAH (significantly elevated 17-OH progesterone)
- Progesterone deficiency combined with hyperandrogenism (PCOS)
This article is for informational purposes only and does not replace professional medical advice. Progesterone is interpreted in the context of cycle day, estradiol, FSH, LH, and prolactin.
For informational purposes only
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Please consult a healthcare professional for medical guidance.