FSH: Normal Levels in Women and Men, Causes of Abnormalities
Reviewed by the LabReadAI medical team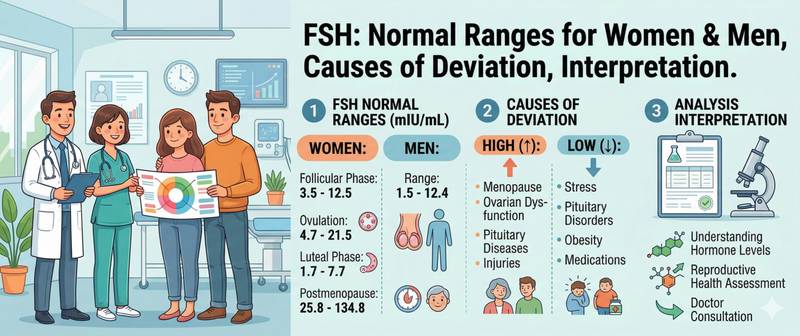
Every menstrual cycle begins with a question the pituitary asks the ovaries: is there a follicle ready to grow? To ask it, the pituitary releases follicle-stimulating hormone. FSH is the conductor of the reproductive orchestra in both sexes — in women it triggers egg maturation, in men it sustains sperm production. When something goes wrong in the pituitary–gonad–sex hormone axis, FSH either climbs high, signalling that the gonads are failing to respond, or falls low, pointing to a problem in the brain itself. Here is how to read this marker correctly.
What Is Follicle-Stimulating Hormone (FSH) and How It Works
FSH (follicle-stimulating hormone) is a glycoprotein hormone produced by the anterior pituitary gland. It is part of the hypothalamus–pituitary–gonad (HPG) axis: the hypothalamus releases gonadotropin-releasing hormone (GnRH) in pulsatile bursts, which drives FSH secretion from the pituitary.
In women, FSH acts on granulosa cells of ovarian follicles, stimulating their growth and oestradiol production. As the follicle matures, rising oestradiol suppresses further FSH release via negative feedback. Then comes a brief positive feedback surge, followed by an LH peak — and ovulation. After ovulation, FSH falls again.
In men, FSH acts on Sertoli cells in the testes, maintaining spermatogenesis. Unlike women, in whom FSH fluctuates cyclically, in men it is relatively stable across hours and months.
This feedback mechanism explains the core interpretive principle: high FSH = the pituitary is shouting because the gonads are not responding. Low FSH = the pituitary is silent because either no signal is coming from above, or sex hormone levels are already sufficient. This distinction is the key to differentiating types of hypogonadism.
Normal FSH Levels in Women, Men and Menopause
FSH norms in women depend substantially on cycle phase — which is why a result without the cycle day specified is nearly uninterpretable.
| Group | Normal FSH, IU/L |
|---|---|
| Women, follicular phase (days 2–5) | 3.5–12.5 |
| Women, ovulatory peak (mid-cycle) | 4.7–21.5 |
| Women, luteal phase | 1.7–7.7 |
| Women, postmenopause | 25.8–134.8 |
| Men 18–70 years | 1.5–12.4 |
| Children under 1 year | < 3.5 |
| Pre-pubertal (3–10 years) | 0.3–4.6 |
| Puberty (11–18 years) | gradual rise to adult levels |
Reference ranges at your specific laboratory may differ. Always use the values printed on your own lab report.
Two key observations:
Postmenopausal norms are in a different category. After ovarian function ceases, the feedback loop disappears — the pituitary raises FSH without restraint. Values of 25–135 IU/L in a woman over 50 are normal, not pathological. Confusion arises when menopausal status is not noted on the test request.
In men, FSH is stable. No need to account for time of day or cycle timing — a fasting morning sample on any day is sufficient.
When to Test FSH in the Cycle and How to Prepare
Correct timing is critically important and is frequently overlooked when the test is ordered.
Women with a regular cycle. Blood should be drawn on cycle days 2–5 (day 1 = the first day of menstrual bleeding). The basal FSH level at the start of the follicular phase is what reflects ovarian reserve: the higher the basal FSH, the lower the reserve. Testing in other cycle phases can return a normal result even when the reserve is diminished.
Women with an irregular cycle or amenorrhoea. Testing can be done on any day — there is no cycle to track. The FSH:LH ratio is interpreted in conjunction with oestradiol.
Men. No strict timing requirements, but morning fasting samples are standard for consistency.
General rules. Blood is drawn fasting (8–12 hours). Avoid intense physical and emotional stress for 3 days before the test — stress activates the HPG axis and can transiently shift gonadotropin levels. Hormonal medications (oral contraceptives, FSH/LH preparations) should be paused for approximately one month before testing if clinically possible, in agreement with the treating physician.
Never test FSH alone. Without simultaneous measurement of LH, oestradiol and TSH, an FSH result tells only half the story. Hypothyroidism is a common and easily missed cause of cycle disturbances that mimics hormonal imbalance.
High FSH Causes in Women, Menopause and Men
High FSH is a signal that the pituitary is trying harder than usual to stimulate the gonads — because they are not responding normally. This is always a "peripheral" type of disorder: the problem lies in the gonads themselves, not in the pituitary.
| Cause in women | Mechanism |
|---|---|
| Physiological menopause | Depletion of the follicular pool → no negative feedback from oestradiol |
| Premature ovarian insufficiency (POI) | Same mechanism but before age 40 — autoimmune, genetic or iatrogenic |
| Turner syndrome (45,X) | Congenital absence of normal ovarian tissue |
| Diminished ovarian reserve | Basal FSH > 10–12 IU/L on cycle day 3 — marker of reduced reserve |
| Chemotherapy and radiotherapy | Gonadotoxic damage to the ovaries |
| Smoking | Accelerates depletion of the follicular pool |
| Cause in men | Mechanism |
|---|---|
| Primary hypogonadism (Klinefelter syndrome, orchitis, trauma) | Testicular damage → reduced negative feedback from inhibin B |
| Untreated cryptorchidism | Undescended testis with impaired spermatogenesis |
| Non-obstructive azoospermia | Primary spermatogenic failure |
| Chemotherapy and radiotherapy | Direct gonadotoxic effect |
| Significant varicocele | Impaired testicular thermoregulation → reduced spermatogenesis |
A specific clinical situation: FSH > 40 IU/L in a woman under 40 without pregnancy or exogenous hormones. This is the criterion for premature ovarian insufficiency (POI) — a condition requiring confirmation by two measurements four weeks apart and urgent referral to a reproductive specialist.
Low FSH Causes: Hypogonadism and Fertility Implications
Low FSH means the pituitary is not generating sufficient signal to the gonads. This is a "central" type of disorder — the problem lies above the level of the ovaries or testes.
- Pregnancy — human chorionic gonadotropin suppresses FSH and LH secretion physiologically; low FSH with a missed period is a reason to perform a pregnancy test first
- Hypothalamic amenorrhoea — significant weight loss, intense training or chronic stress reduces GnRH pulse frequency → FSH and LH fall
- Hyperprolactinaemia — excess prolactin suppresses GnRH → secondarily reduces FSH and LH; pituitary tumour (prolactinoma) is a common cause
- Pituitary tumour or damage — adenoma, head injury, Sheehan's syndrome (pituitary necrosis after postpartum haemorrhage)
- Exogenous sex hormone use — oral contraceptives, anabolic steroids, testosterone preparations suppress FSH via negative feedback
- Kallmann syndrome — congenital GnRH deficiency combined with anosmia
FSH-to-LH Ratio in PCOS and Ovarian Reserve Assessment
FSH is never interpreted without LH. The ratio of these two gonadotropins carries clinically valuable information beyond the absolute values of each.
In PCOS, the LH:FSH ratio > 2–3:1 with normal or mildly reduced absolute FSH is the classic pattern. The pituitary releases disproportionately high LH relative to FSH, driving the ovaries to produce androgens instead of achieving normal follicular maturation. In PCOS, this imbalance is one of the central pathogenetic mechanisms.
In menopause, both gonadotropins rise sharply, but FSH rises faster and higher — the LH:FSH ratio falls below 1. In menopause, FSH > 40 IU/L combined with amenorrhoea for more than 12 months is the laboratory criterion for postmenopause.
In primary male hypogonadism, both gonadotropins are elevated, but the pattern of their ratio helps distinguish isolated spermatogenic failure (FSH rises more, LH relatively normal) from total testicular failure (both elevated proportionally).
In hypothalamo-pituitary insufficiency, both gonadotropins are low or at the lower limit of normal — isolated reduction of one without the other is uncommon and warrants particular alertness.
FSH Blood Test Interpretation: When to See a Doctor Urgently
- FSH > 25 IU/L in a woman under 40 without pregnancy or hormone use — suspected premature ovarian insufficiency; requires urgent confirmation and reproductive specialist referral
- FSH > 12 IU/L on cycle day 3 when pregnancy is planned — significant diminished ovarian reserve; assessment of IVF and ovulation induction prospects cannot be delayed
- Very low FSH (< 1 IU/L) with amenorrhoea — exclude prolactinoma and other pituitary tumours; MRI of the brain required
- Absent puberty by age 13–14 in girls or 14–15 in boys with low FSH — constitutional delay or hypogonadotropic hypogonadism; differential diagnosis by a paediatric endocrinologist
- Sudden FSH rise in a patient who received chemo- or radiotherapy — marker of gonadotoxic damage; reproductive prognosis assessment needed
FSH is a precise navigator in a complex hormonal system — but only when drawn at the correct time and interpreted in context with the other markers. Interpreting it without knowing the cycle phase, LH and oestradiol levels is like reading a compass without knowing which hemisphere you are in.
For FSH reference ranges in women after 40, perimenopause signs and the full hormone panel, see the article which hormone tests women should get after 40.
This article is for informational purposes only. Interpretation of test results and diagnosis are the responsibility of a qualified physician.
For informational purposes only
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Please consult a healthcare professional for medical guidance.