TSH Thyroid-Stimulating Hormone: Normal Range and Causes
Reviewed by the LabReadAI medical team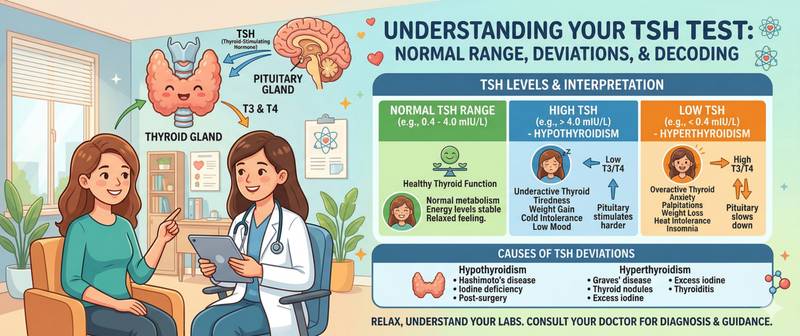
TSH — thyroid-stimulating hormone — occupies a unique position among hormonal markers: it simultaneously reflects the state of the thyroid gland and actively controls it. This is why TSH is among the first tests ordered for fatigue, weight gain, hair loss, or heart rhythm disturbances — symptoms that may or may not point to thyroid pathology. Understanding the biology of this hormone is the foundation of interpreting its values correctly.
What TSH Is and How It Regulates the Thyroid
TSH is a glycoprotein hormone produced by thyrotroph cells in the anterior pituitary. Its structure resembles other pituitary gonadotropins (LH, FSH) and human chorionic gonadotropin (hCG): all share a common α-subunit and a hormone-specific β-subunit that determines biological activity.
TSH regulation operates on a negative feedback loop:
- The hypothalamus releases thyrotropin-releasing hormone (TRH), stimulating the pituitary to produce TSH
- The pituitary releases TSH into the bloodstream, where it reaches the thyroid gland
- The thyroid gland, under TSH stimulation, synthesizes thyroxine (T4) and triiodothyronine (T3)
- T3 and T4 feed back to inhibit TSH production by the pituitary
This is the classic loop: the fewer thyroid hormones in circulation, the higher the TSH (the pituitary presses the accelerator); the more thyroid hormones, the lower the TSH (the pituitary releases the pressure). This is precisely why TSH is a more sensitive indicator of thyroid dysfunction than T3 or T4 themselves — it reacts earlier, even while peripheral hormone levels are still technically normal.
TSH binds to specific receptors on thyroid cells (thyrocytes) and serves two functions: it stimulates synthesis and secretion of thyroid hormones, and it drives growth of thyroid tissue. With chronically elevated TSH, the thyroid gland gradually enlarges — a goiter forms.
A full practical guide to interpreting TSH results across different clinical situations is available in the article how to read TSH results.
TSH Normal Ranges by Age and Physiological State
TSH reference values vary substantially with age and physiological condition. Applying an adult reference range to a newborn or a pregnant woman is a significant interpretive error.
| Age / condition | Normal TSH (mIU/L) |
|---|---|
| Newborns days 1–4 | 1.0–39.0 |
| Infants under 6 weeks | 1.7–9.1 |
| Infants 6 weeks – 14 months | 0.7–6.4 |
| Children 14 months – 5 years | 0.7–5.97 |
| Children 5–14 years | 0.6–4.84 |
| Adults 18–60 years | 0.4–4.0 |
| Adults over 60 years | 0.5–8.0 |
| Pregnancy — 1st trimester | 0.1–2.5 |
| Pregnancy — 2nd trimester | 0.2–3.0 |
| Pregnancy — 3rd trimester | 0.3–3.5 |
Several important nuances:
Adults over 60. The upper limit of normal is higher in older adults than in young adults — this is physiologically normal and does not require treatment. Prescribing thyroid hormones to an elderly patient with a TSH of 5–6 mIU/L based solely on the laboratory value without symptoms is a recognized and undesirable clinical error.
Pregnancy. The lower reference range in the first trimester reflects the fact that hCG — the pregnancy hormone — partially mimics TSH and directly stimulates the thyroid, reducing the need for pituitary-derived TSH. This is not pathological.
Diurnal rhythm. TSH follows a distinct circadian pattern: peak levels occur between 2–4 AM and early morning (6–8 AM); nadir is in the afternoon (12–18 hours). The difference between morning and afternoon values can be 1.5 to 2-fold — which explains why morning testing is recommended.
How to Prepare for a TSH Blood Test
TSH is considered a relatively stable hormone, but several conditions significantly influence the result.
- Optimal testing time: morning, 8:00–11:00 AM, fasting or 3–4 hours after a light breakfast
- For serial monitoring: always test under identical conditions (same time of day, same laboratory, same dietary status) — different analytical methods can produce results differing by 0.2–0.5 mIU/L
- When taking levothyroxine: draw blood before the morning dose; otherwise the result reflects the drug's peak level, not the true background TSH
- Acute illness, surgery, and hospitalization can transiently suppress TSH — repeat testing after recovery
TSH is almost always ordered as part of the full thyroid panel — free T4 and free T3 — and with thyroid peroxidase antibodies when autoimmune disease is suspected.
High TSH: Causes and Clinical Significance
Elevated TSH means the pituitary is intensively stimulating the thyroid — a response to insufficient production of thyroid hormones or a disruption of their feedback effect at the pituitary level.
Primary hypothyroidism is the most common cause. The thyroid produces inadequate T4 and T3 → the pituitary compensatorily increases TSH. Causes include Hashimoto's autoimmune thyroiditis (most prevalent), thyroidectomy (including for thyroid cancer), radioiodine treatment, iodine deficiency, and congenital hypothyroidism. Clinical details and treatment are covered in hypothyroidism.
Subclinical hypothyroidism — TSH elevated (typically 4–10 mIU/L) with normal T4 and minimal or absent symptoms. Requires monitoring but not always treatment.
Thyroid hormone resistance — a rare genetic condition: thyroid hormone receptors are insensitive to T3 and T4; the pituitary does not register normal concentrations and continues secreting TSH. Characteristic combination: elevated TSH alongside simultaneously elevated T4 and T3.
TSH-secreting pituitary adenoma — a rare cause of elevated TSH. Distinguishing feature from primary hypothyroidism: T4 is also elevated, not reduced.
Transient causes: euthyroid sick syndrome during recovery from systemic illness, adrenal insufficiency, and medications (amiodarone, lithium, metoclopramide, certain antipsychotics).
Low TSH: Causes and Clinical Significance
Suppressed TSH means the pituitary has gone quiet — the thyroid is overproducing hormones or receiving stimulation that bypasses the normal regulatory loop.
Hyperthyroidism (thyrotoxicosis) is the primary cause of suppressed TSH. Graves' disease: antibodies mimic TSH, autonomously stimulating the thyroid. Toxic nodular goiter: individual nodules function independently of TSH. In overt thyrotoxicosis, TSH is often undetectable (< 0.01 mIU/L). Details in hyperthyroidism.
Subclinical thyrotoxicosis — TSH suppressed (< 0.4 mIU/L), T4 and T3 normal, minimal symptoms. In older adults, increases the risk of atrial fibrillation and bone density loss.
Levothyroxine overdose — when hypothyroidism is treated with too high a dose. A common iatrogenic cause.
Central hypothyroidism (secondary/tertiary) — pituitary or hypothalamic pathology. Paradoxical combination: TSH low or "normal" while T4 is also low. Causes: pituitary tumors, ischemia, infiltrative disease, head trauma.
First trimester of pregnancy — physiological TSH suppression from hCG stimulation.
Transient causes: acute illness, fasting, high-dose glucocorticoids, dopaminergic medications.
What Affects TSH Levels: Drugs and Physiological Factors
TSH is sensitive to a wide range of external influences — an essential consideration when interpreting borderline results.
Drugs that raise TSH:
- Amiodarone — contains iodine and directly disrupts thyroid metabolism; TSH may rise even with normal thyroid function
- Lithium — concentrates in the thyroid, suppresses thyroid hormone synthesis
- Metoclopramide, domperidone — dopamine antagonists, indirectly stimulate TSH secretion
- Certain antipsychotics (haloperidol, chlorpromazine)
Drugs that lower TSH:
- High-dose glucocorticoids — suppress TRH and TSH secretion
- Dopamine and bromocriptine — direct inhibitors of pituitary thyrotrophs
- Excess levothyroxine or triiodothyronine
- High-dose biotin (vitamin B7) — a technical artifact: does not change actual TSH but interferes with immunoassay methods, producing falsely low readings
Physiological factors:
- Acute psychological stress — transient decrease
- Fasting — TSH reduction
- Estradiol and pregnancy — reduction via hCG action and direct estrogen effects on the pituitary
- Obesity — modest TSH elevation in some patients even without thyroid pathology
- Biotin: if the patient takes high doses, blood should be drawn 48–72 hours after the last dose
When TSH Levels Require Medical Attention
Minor borderline deviations without symptoms often require only monitoring — not treatment. Clinical approach depends on the combination of the TSH value, symptoms, and T4/T3 results.
See a doctor soon if you have:
- TSH > 4.0 mIU/L with symptoms (fatigue, cold intolerance, weight gain, hair loss)
- TSH > 10 mIU/L — regardless of symptoms
- TSH < 0.1 mIU/L — regardless of symptoms
- Any TSH deviation during pregnancy
- TSH trending up or down on serial testing without an obvious explanation
Seek urgent care if symptoms of thyrotoxic crisis appear — high fever, escalating heart rate > 140 bpm, agitation, or altered consciousness — or myxedema coma: marked lethargy, hypothermia, and edema in a patient with known hypothyroidism.
TSH is a key marker in women's hormonal health screening: deviations affect the menstrual cycle, weight and general wellbeing. For the full hormone panel, see the article which hormone tests women should get after 40.
This article is for informational purposes only and does not replace professional medical advice. TSH interpretation should be performed by an endocrinologist or GP in the context of the full clinical picture.
For informational purposes only
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Please consult a healthcare professional for medical guidance.