LH: Normal Levels in Women and Men, Causes of Abnormalities
Reviewed by the LabReadAI medical team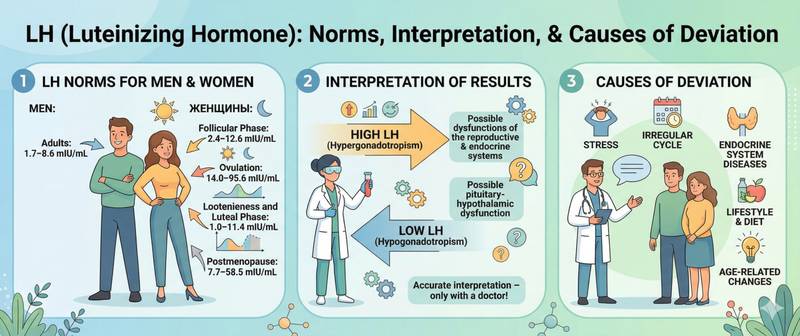
If the reproductive system were a rocket launch, FSH would be the command to "fuel and prepare" — and luteinising hormone would be the button marked "launch." It is the mid-cycle LH surge that sends the signal causing the mature follicle to rupture and release the egg. Every home ovulation test is built around detecting precisely this LH peak. In men, LH is equally essential: it orders Leydig cells in the testes to synthesise testosterone. Understanding LH means understanding how two fundamental hormonal mechanisms work — and how abnormalities in LH levels can disrupt both fertility and hormonal balance.
What Is LH and How It Differs from FSH
LH (luteinising hormone) is a glycoprotein hormone produced by the anterior pituitary gland, just like FSH. Both are regulated by pulsatile GnRH release from the hypothalamus, and both act on the gonads — but their roles are fundamentally different.
Where FSH is the hormone of growth and maturation (building the follicle in women, sustaining spermatogenesis in men), LH is the trigger hormone and steroid synthesis hormone.
In women, LH has two tasks:
- At mid-cycle, when a mature follicle produces a peak of oestradiol, a positive feedback loop fires — the pituitary responds with a powerful LH surge. This burst ruptures the follicle and initiates ovulation within 36–44 hours.
- After ovulation, LH supports the corpus luteum — the temporary gland that forms at the site of the ruptured follicle. The corpus luteum synthesises progesterone, essential for sustaining an early pregnancy.
In men, LH acts on Leydig cells in the testes, stimulating testosterone synthesis. The feedback loop works precisely: sufficient testosterone → LH falls → synthesis brakes. Too little testosterone → LH rises → Leydig cells activate.
This is why male hypogonadism always requires measuring testosterone and LH together: high LH with low testosterone = primary problem in the testes (the pituitary is shouting, the testes are not listening); low LH with low testosterone = secondary problem in the pituitary or hypothalamus.
Normal LH Levels in Blood
Like FSH, LH in women changes throughout the cycle — and far more dramatically: the difference between the basal level and the ovulatory peak is 5–10 fold.
| Group | Normal LH, IU/L |
|---|---|
| Women, follicular phase (days 2–7) | 2.4–12.6 |
| Women, ovulatory peak | 14.0–95.6 |
| Women, luteal phase | 1.0–11.4 |
| Women, postmenopause | 7.7–58.5 |
| Men 18–70 years | 1.7–8.6 |
| Children under 1 year | < 3.0 |
| Pre-pubertal (3–10 years) | < 0.5 |
| Puberty (11–18 years) | gradual rise |
Reference ranges at your specific laboratory may differ. Always use the values printed on your own lab report.
A few important observations:
The ovulatory peak is a diagnostic trap. If blood happens to be drawn on the day of ovulation, LH levels can be 5–10 times higher than the "normal" basal level. Without knowing the cycle phase, such a result is easily mistaken for abnormalities. This is precisely why basal LH is always measured in the follicular phase (days 2–7).
Postmenopause. After ovarian function ceases, LH rises — but less dramatically than FSH. A FSH:LH ratio > 1 in postmenopause is physiological. If LH exceeds FSH in postmenopause — a gonadotropin-secreting tumour should be excluded.
Pre-puberty. In children before puberty, LH levels are barely detectable (< 0.5 IU/L) — the GnRH system is in deep dormancy. A significant LH rise in a child below age 8–9 is one of the criteria for precocious puberty, and such abnormalities warrant immediate evaluation.
How to Prepare for an LH Blood Test
The rules are nearly identical to FSH — logically so, since they are almost always ordered together.
Women with a regular cycle. Basal LH on cycle days 2–7, on the same day as FSH. This avoids sampling during the ovulatory peak and allows accurate calculation of the LH:FSH ratio.
Home ovulation tests. Over-the-counter ovulation tests detect the urinary LH peak — which precedes ovulation by 24–36 hours. Testing begins 3–4 days before the estimated mid-cycle and is performed daily at the same time (preferably 14:00–18:00). In PCOS, home ovulation tests are unreliable — chronically elevated basal LH produces false-positive lines.
Men. Morning fasting sample on any day; LH in men is sufficiently stable.
General rules. Blood drawn fasting (8–12 hours). Avoid intense physical and emotional stress for 3 days prior. Hormonal preparations containing oestradiol, progesterone or testosterone suppress LH via negative feedback — pause for approximately one month before testing if clinically feasible, in agreement with the physician.
LH without FSH is an incomplete test. Only together do they provide the picture needed for diagnosis.
Elevated LH: Causes
| Cause in women | Mechanism |
|---|---|
| Menopause and postmenopause | Loss of oestradiol feedback → both gonadotropins rise |
| Premature ovarian insufficiency | Same mechanism before age 40 |
| PCOS | Disrupted GnRH pulsatility → chronically high LH with relatively normal FSH; LH:FSH > 2 |
| Turner syndrome | Primary gonadal failure |
| Ovulatory peak | Physiological; not pathological when sampled at mid-cycle |
| Cause in men | Mechanism |
|---|---|
| Primary hypogonadism | Reduced testosterone → no feedback suppression → LH rises |
| Klinefelter syndrome (47,XXY) | Congenital Leydig cell dysfunction |
| Orchitis, testicular trauma | Acquired testicular tissue damage |
| Androgen resistance | Tissues do not respond to testosterone → LH not suppressed by feedback |
A specific case — isolated high LH with normal FSH in a woman outside the ovulatory peak. This is the classic PCOS pattern. In PCOS, the pituitary produces LH at an accelerated pulse rate while FSH remains moderate. The ovaries receive a signal to "make androgens" instead of "mature a follicle." In PCOS, an LH:FSH ratio > 2–3:1 is seen in 60–70% of patients and is a useful diagnostic pointer, although it is not part of the official Rotterdam criteria.
Low LH: Causes
Low LH is always a "signal from above": the problem lies in the pituitary or hypothalamus, not in the gonads.
- Pregnancy — hCG suppresses LH and FSH physiologically; the first thing to exclude when LH is low with a missed period
- Hypothalamic amenorrhoea — energy deficit (anorexia, extreme dieting), chronic stress, intensive sport reduce GnRH pulse frequency; LH and FSH fall proportionally
- Hyperprolactinaemia — excess prolactin suppresses GnRH → secondary LH reduction; always check prolactin when central hypogonadism is suspected
- Pituitary tumours and damage — adenoma, craniopharyngioma, radiation injury, Sheehan's syndrome
- Kallmann syndrome — congenital GnRH deficiency; LH and FSH are at zero from birth
- Exogenous androgens and anabolic steroids — high exogenous testosterone suppresses LH → testes stop producing endogenous testosterone → atrophy; a common cause in men using steroids without medical supervision
LH and FSH: The Ratio in Clinical Practice
The LH:FSH ratio is one of the most frequently used diagnostic indices in reproductive endocrinology. It is calculated by dividing the LH value by the FSH value, both measured in the follicular phase.
| LH:FSH ratio | Clinical significance |
|---|---|
| 0.5–1.5 (normal range) | Physiological in follicular phase |
| > 2.0–3.0 in a woman outside the peak | Characteristic of PCOS — requires further investigation |
| < 0.5 when both values are low | Hypothalamo-pituitary insufficiency |
| LH > FSH in postmenopause at normal FSH | Exclude LH-secreting tumour |
| FSH >> LH when both are high | Primary gonadal failure (menopause, POI) |
A practical example. A 32-year-old woman with irregular cycles: LH = 18.4 IU/L, FSH = 6.1 IU/L, oestradiol normal. LH:FSH ratio = 3.0. Combined with polycystic ovarian morphology on ultrasound and mild hirsutism — the picture fits PCOS. If instead both gonadotropins were below 1.0 IU/L — prolactin and a pituitary MRI would be the next steps.
In menopause, the ratio is interpreted differently: both gonadotropins are high, but FSH should exceed LH. If a postmenopausal woman's LH unexpectedly exceeds her FSH — this is atypical and warrants investigation.
When to See a Doctor Urgently
- LH > 40 IU/L in a woman under 40 outside the ovulatory peak — suspected premature ovarian insufficiency; urgent referral to a reproductive specialist
- LH:FSH > 3 with irregular cycles — probable PCOS with significant hormonal imbalance; planned but prompt gynaecological-endocrinological assessment
- Very low LH (< 0.5 IU/L) with amenorrhoea in a non-pregnant woman — exclude prolactinoma; pituitary MRI mandatory
- Low LH with low testosterone in a man — secondary hypogonadism; neuroimaging and endocrinologist consultation required
- Elevated LH in a girl below age 8 or a boy below age 9 — criterion for precocious puberty; paediatric endocrinologist without delay
- Sudden rise in LH and FSH in a patient after chemotherapy or radiotherapy — gonadotoxic damage assessment; reproductive prognosis evaluation needed
LH is the hormone of action where FSH is the hormone of preparation. The first triggers ovulation and sex hormone synthesis; the second grows the follicle and supports spermatogenesis. Together they form a diagnostic pair without which reproductive abnormalities cannot be fully decoded — and interpreting LH levels in isolation is never sufficient.
This article is for informational purposes only. Interpretation of test results and diagnosis are the responsibility of a qualified physician.
For informational purposes only
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Please consult a healthcare professional for medical guidance.