PSA Blood Test: Normal Levels by Age, Results and Causes
Reviewed by the LabReadAI medical team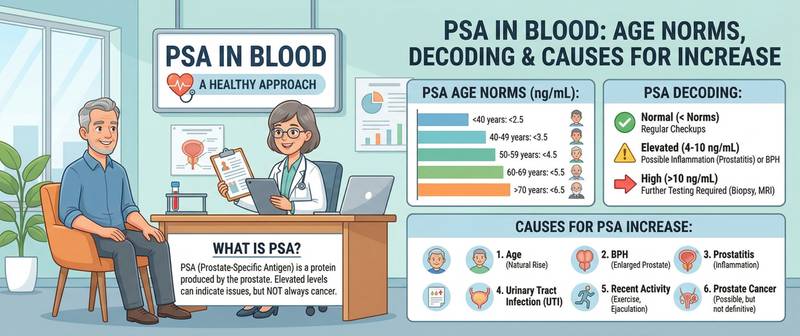
A man receives a PSA result above the reference range and immediately fears the worst. In reality, elevated PSA is far more often a benign finding than a cancer signal — it rises with prostate enlargement, inflammation, physical pressure on the gland and even a bicycle ride. Prostate-specific antigen is a sensitive but non-specific marker: distinguishing a benign process from a malignant one requires the right context, trends over time and additional tests.
What Is PSA and Why Is It Measured?
Prostate-specific antigen is a glycoprotein produced by the epithelial cells lining the prostate gland. Under normal conditions a small amount enters the bloodstream — this is physiological. A sharp rise occurs when the barrier between prostate tissue and blood vessels is disrupted: by inflammation, mechanical trauma or tumour growth.
Biologically, PSA liquefies seminal fluid after ejaculation. Diagnostically, it serves as an indicator of prostate health: blood levels reflect the gland's volume, the presence of inflammation and the likelihood of malignant disease.
PSA is measured for: prostate cancer screening in men over 45–50; monitoring after prostate cancer treatment (surgery, radiotherapy, hormone therapy); diagnosing chronic prostatitis; and tracking benign prostatic hyperplasia (BPH). As part of comprehensive urological screening, PSA is a standard component of the tumour marker panel.
PSA Normal Ranges by Age
PSA rises physiologically with age as the prostate gradually enlarges — even without pathology, more antigen is secreted. Age-specific reference ranges are therefore essential.
| Age | Normal total PSA (ng/mL) |
|---|---|
| 40–49 years | < 2.5 |
| 50–59 years | < 3.5 |
| 60–69 years | < 4.5 |
| 70 years and over | < 6.5 |
A level above 4 ng/mL is the traditional biopsy referral threshold, but contemporary guidelines increasingly favour an individualised approach accounting for age, rate of change and the free-to-total PSA ratio. A level above 10 ng/mL substantially increases the probability of malignancy and almost always indicates the need for biopsy.
Beyond the absolute value, rate of change matters: PSA velocity (PSAV) above 0.75 ng/mL per year is considered a warning sign regardless of the absolute level.
Free PSA vs Total PSA: What Matters More for Diagnosis?
PSA circulates in blood in two forms: bound to plasma proteins and unbound (free). The combined concentration is total PSA. Free PSA is measured separately, and their ratio is calculated.
Free PSA index = (free PSA / total PSA) × 100%
| Free PSA index | Interpretation |
|---|---|
| > 25% | Cancer unlikely — BPH or prostatitis more probable |
| 15–25% | Grey zone — further monitoring needed |
| < 15% | Elevated risk of malignant process |
| < 10% | High probability of prostate cancer |
In prostate cancer, tumour cells predominantly secrete bound PSA — the free fraction falls. In BPH, the free fraction is proportionally higher. The index is most useful in the 4–10 ng/mL range, where the absolute PSA value alone is insufficient to decide about biopsy.
Causes of Elevated PSA
High PSA is not synonymous with cancer. Any disruption of the barrier between prostate tissue and bloodstream raises the marker.
Benign causes are far more common than malignant ones. Benign prostatic hyperplasia is the most frequent: an enlarged gland produces more PSA proportional to its volume without any inflammation. Acute and chronic prostatitis raises PSA sharply — sometimes to 50–100 ng/mL in bacterial infection, creating a false alarm that resolves within weeks of treatment. Mechanical interventions — prostate biopsy, cystoscopy, catheterisation — elevate PSA for days to weeks; the test should not be performed until at least four to six weeks after these procedures.
Physiological triggers include ejaculation (moderate transient rise for 24–48 hours), cycling (perineal pressure), and intense physical exercise — all producing short-lived elevation without pathology.
Prostate cancer — the malignant cause. PSA in cancer typically rises faster and is accompanied by a falling free PSA index. In bone metastases, alkaline phosphatase rises simultaneously — an additional marker evaluated in parallel. When prostatic obstruction causes hydronephrosis, rising creatinine signals impaired kidney function and requires urgent urological intervention.
How to Prepare for a PSA Blood Test
Preparation rules for PSA are stricter than for most biochemical tests because physiological factors genuinely distort results.
Two days before the test: abstain from sexual activity and ejaculation; avoid cycling, motorcycling and gym equipment that compresses the perineum; refrain from intense physical exertion. Fast for at least 8 hours — blood is drawn in the morning. After medical procedures: wait 48 hours after digital rectal examination, one week after urinalysis with catheterisation, and four to six weeks after prostate biopsy or surgery. Declare all medications: finasteride and dutasteride halve PSA levels — without accounting for this, a doctor may significantly underestimate the true value.
For serial monitoring, always use the same laboratory and test at the same time of day: inter-laboratory calibration differences can produce up to 20% discrepancy that mimics a real change in PSA.
Interpreting Results: What to Do With a High PSA
The appropriate response depends on the specific value and clinical context.
PSA 0–4 ng/mL (age-adjusted) — annual monitoring from age 50 (from 45 with a family history of prostate cancer). PSA 4–10 ng/mL — grey zone: measure the free PSA index and consult a urologist. Biopsy is indicated when the index is below 15% or PSA velocity is high. PSA > 10 ng/mL — high probability of malignancy; urological review within days is mandatory. PSA > 20 ng/mL — possible extracapsular spread; staging workup includes pelvic MRI and bone scintigraphy.
After radical prostatectomy, PSA should be undetectable (< 0.1 ng/mL). Any measurable rise indicates recurrence and requires immediate oncological assessment.
When High PSA Requires Urgent Medical Attention
A scheduled urology appointment is appropriate for most cases of mild PSA elevation. Certain situations, however, cannot wait.
See a doctor within days if: PSA exceeds 10 ng/mL on a first measurement; PSA rises by more than 2 ng/mL in a year during surveillance; PSA becomes detectable after prostate cancer treatment.
Seek emergency care or call emergency services if: urinary retention develops alongside high PSA and perineal pain; signs of sepsis appear with acute prostatitis (high fever, rigors, altered consciousness); bone pain combined with sharply rising PSA suggests metastatic disease.
Conclusion
PSA is a powerful tool for early prostate cancer detection, but it is far from absolute: an elevated result is more often a benign process than malignancy. The decision to proceed to biopsy is made on the basis of multiple factors — the absolute value, trend over time, free PSA index, MRI findings and the clinical picture. Self-interpretation of PSA without a urologist is not advisable. Regular PSA screening from age 45–50 remains one of the most effective strategies for catching prostate cancer when it is still curable.
For informational purposes only
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Please consult a healthcare professional for medical guidance.