Urinalysis (UA): Indicators, Normal Values and Interpretation
Reviewed by the LabReadAI medical team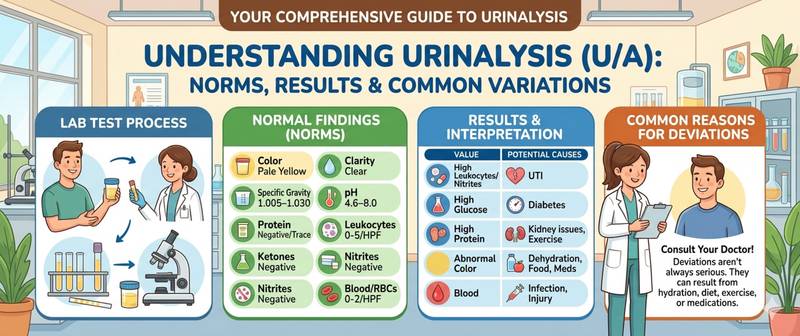
You get a results sheet with two dozen rows — color, pH, protein, leukocytes, casts — and not a single number speaks for itself. A urinalysis (UA) is one of the most commonly ordered laboratory tests, capable of pointing to kidney inflammation, diabetes, urinary tract infections, and even liver problems before obvious symptoms appear. This article walks through every indicator: what it measures, what a normal result looks like, and what deviations mean. For a step-by-step walkthrough of your personal results, see how to read a urinalysis.
What Is a Urinalysis and Why Is It Ordered?
A UA is a comprehensive laboratory test that evaluates the physical properties of urine, its chemical composition, and the cellular sediment under a microscope. These three components together provide a full picture of kidney and urinary tract function, and indirectly reflect metabolic and immune status.
A doctor orders a UA in several situations:
- Routine health screening or annual checkup
- Symptoms such as painful urination, increased frequency, or changes in urine color
- Monitoring treatment of cystitis, pyelonephritis, or urinary stones
- Ongoing management of diabetes, hypertension, or pregnancy
- Pre-operative evaluation
The test takes 1–2 hours in the lab and requires no special preparation beyond correct sample collection.
How to Collect the Sample: Preparation for a Urinalysis
Collection errors are the most common cause of false results. Contamination of the sample with epithelial cells, bacteria, or secretions makes the analysis unreliable — and means the test has to be repeated.
Collection guidelines:
- Collect the first morning void — the most concentrated sample, reflecting kidney function at rest.
- Clean the genital area thoroughly beforehand, without antibacterial soap.
- Let the first 1–2 seconds of urine pass into the toilet, then catch the midstream portion in a sterile container.
- Volume: at least 30–50 mL.
- Use a pharmacy-grade sterile container, not a jar from home.
- Deliver to the lab within 1–2 hours. Refrigerator storage is acceptable for up to 4 hours; longer than that distorts results.
Women should avoid collecting urine during menstruation — blood will contaminate the sample and produce false positives for red blood cells and protein. If the test is urgent, use a tampon.
Physical Properties of Urine: Color, Clarity, Odor, and Density
The lab technician evaluates these parameters visually and with a urinometer before chemical analysis. They provide the first overall impression of the sample.
Color is normally straw-yellow to amber. Intensity depends on hydration: the less fluid consumed, the darker the urine. Deviations:
- Red or brown — blood (hematuria), beets, certain medications
- Dark brown, "beer-colored" — bilirubinuria, liver disease
- Cloudy white — pus in severe infection
- Nearly colorless — excessive fluid intake or diabetes insipidus
Clarity is normally full. Turbidity suggests the presence of bacteria, leukocytes, mucus, or salt crystals.
Odor is normally mild and specific. An ammonia smell indicates bacterial decomposition. An acetone smell suggests ketoacidosis, characteristic of decompensated diabetes.
Specific gravity (1.010–1.025) reflects the kidney's ability to concentrate urine. Persistently low density is a sign of chronic kidney insufficiency or diabetes insipidus.
pH is normally 4.5–8.0. Strongly acidic urine occurs with a high-meat diet and gout; alkaline urine with urinary tract infections and a vegetarian diet.
Chemical Indicators in a Urinalysis: Normal and Abnormal
A dipstick test detects in seconds the presence or absence of key substances that should not normally appear in urine.
Protein. Normal — absent or trace amounts up to 0.033 g/L. The presence of protein (proteinuria) is one of the most important signs of damage to the kidney filter. Read more: protein in urine — causes, severity levels, and when it is dangerous.
Glucose. Normally absent. Appears when blood sugar exceeds the renal threshold (approximately 9–10 mmol/L) — most commonly in diabetes mellitus.
Ketone bodies. Normally absent. Acetone and other ketones appear during fasting, low-carbohydrate diets, and — critically — diabetic ketoacidosis. More on this indicator: ketones in urine.
Bilirubin. Normally absent. Appears in liver and biliary tract disease.
Urobilinogen. Up to 17 µmol/L is acceptable. Elevated levels suggest hemolysis or impaired liver function.
Nitrites. Normally absent. Appear when bacteria convert urinary nitrates to nitrites. A positive nitrite test is a signal of cystitis or pyelonephritis.
Urine Sediment Microscopy: Cells, Casts, and Crystals
After centrifuging the sample, the lab technician examines the sediment under a microscope. This is the most informative part of the urinalysis.
Leukocytes — normal up to 5 per high-power field in women, up to 3 in men. Exceeding this (pyuria) indicates inflammation in the urinary tract. The higher the count, the more active the process. Everything you need to know: leukocytes in urine.
Red blood cells — normal 0–3 per high-power field. Higher values (hematuria) require investigation: urinary stones, tumors, glomerulonephritis, trauma.
Casts are protein molds formed in the renal tubules. Occasional hyaline casts are acceptable. Granular, waxy, or red blood cell casts indicate serious kidney pathology.
Bacteria — normally absent. Detection in a properly collected sample is an indication for urine culture to identify the organism and its antibiotic sensitivity.
Crystals are salts precipitated out of solution. Occasional oxalate or urate crystals are not pathological. Massive crystalluria with symptoms may suggest urolithiasis.
Epithelial cells — occasional transitional or squamous cells are acceptable. Abundant renal (tubular) epithelium indicates tubular damage.
Urinalysis Normal Values: Summary Table
| Parameter | Normal |
|---|---|
| Color | Straw-yellow |
| Clarity | Clear |
| Odor | Mild, specific |
| pH | 4.5–8.0 |
| Specific gravity | 1.010–1.025 |
| Protein | Absent / up to 0.033 g/L |
| Glucose | Absent |
| Ketone bodies | Absent |
| Bilirubin | Absent |
| Urobilinogen | Up to 17 µmol/L |
| Nitrites | Absent |
| Leukocytes | Up to 5 HPF (women) / 3 HPF (men) |
| Red blood cells | 0–3 per high-power field |
| Hyaline casts | Occasional / absent |
| Bacteria | Absent |
| Epithelial cells | Occasional |
Reference ranges may vary slightly by laboratory method and equipment — always check the reference values on your specific results sheet.
When Urinalysis Results Require Urgent Medical Attention
Most UA abnormalities are mild and warrant a scheduled appointment. But some findings call for prompt evaluation:
- Visible blood in urine, or hematuria above 10–15 red blood cells per field
- Leukocyturia above 30–50 per field — massive inflammation
- Red blood cell or waxy casts — severe kidney pathology
- Protein above 1 g/L, especially combined with edema and elevated blood pressure
- Significant bacteriuria with fever and flank pain — possible pyelonephritis
- Heavy ketonuria with vomiting and altered consciousness — risk of diabetic ketoacidosis
If your UA shows abnormalities for the first time, do not interpret the result on your own. A doctor will evaluate it in the context of your symptoms, history, and other investigations.
Conclusion
A urinalysis is a simple, accessible, and highly informative test. Its three components — physical properties, chemical composition, and sediment microscopy — together paint a picture of kidney and urinary tract function, and sometimes reveal systemic metabolic disorders. The key to an accurate result is correct sample collection. If anything on your results sheet concerns you, consult a general practitioner or urologist — most abnormalities respond well to treatment when caught early.
This content is for informational purposes only and does not replace professional medical advice.
For informational purposes only
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Please consult a healthcare professional for medical guidance.