MCV Blood Test: Normal Range, Causes of Changes and Anaemia Diagnosis
Reviewed by the LabReadAI medical team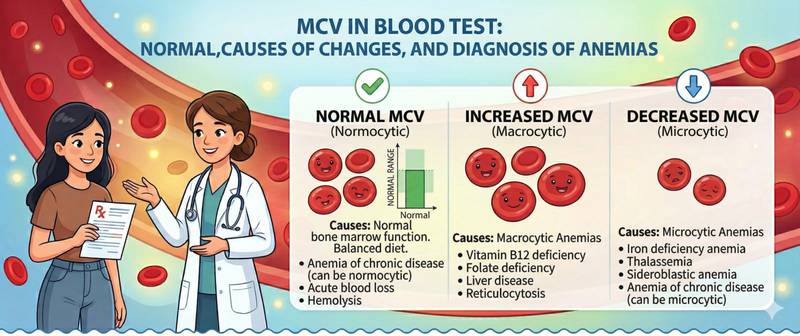
In a complete blood count, the MCV line is often overlooked — especially when haemoglobin is normal. Yet mean corpuscular volume is one of the most informative markers for diagnosing the cause of anaemia: it divides all anaemias into three fundamentally different types, each pointing to its own group of diseases. Without MCV, the doctor has a fact — "haemoglobin is low" — but not an answer — "why."
What Is MCV and Why Is It Measured
MCV (Mean Corpuscular Volume) measures the average size of a red blood cell in femtolitres (fL). Modern haematology analysers calculate it automatically from the ratio of haematocrit to red cell count.
Red cell size is not a random characteristic. It depends directly on how cells mature in the bone marrow: for an erythrocyte to reach normal size, it needs the right amount of haemoglobin (meaning enough iron) and a normal cell division process (meaning adequate vitamin B12 and folate). When either is disrupted, size changes in a predictable way.
This is why MCV is the primary tool for classifying anaemias — the first thing a doctor checks after haemoglobin in a complete blood count.
Normal MCV by Age
| Age | Normal MCV (fL) |
|---|---|
| Newborns | 95–121 |
| 1–6 months | 73–101 |
| 6 months–2 years | 70–86 |
| 2–12 years | 73–89 |
| 12–18 years | 78–95 |
| Adults | 80–100 |
In older adults, the upper MCV limit may be slightly higher due to physiological changes in erythropoiesis. Reference ranges differ slightly between laboratories — always use your specific report's values.
MCV and Anaemia Classification: Three Types
A fall in haemoglobin establishes anaemia as a fact. MCV explains its nature. Three fundamental patterns:
Microcytic anaemia (MCV < 80 fL) — red cells smaller than normal. The cause is almost always impaired haemoglobin synthesis. The most common cause worldwide: iron-deficiency anaemia — insufficient iron to build haem. Less commonly: thalassaemia (inherited globin defect), anaemia of chronic disease (iron is "locked" in stores during prolonged inflammation). When microcytic anaemia is suspected, the next step is an iron panel including ferritin.
Normocytic anaemia (MCV 80–100 fL) — normal-sized red cells, but too few of them. The bone marrow is either not producing enough or cells are being destroyed. Causes: acute blood loss (cell size hasn't yet changed), chronic kidney disease (erythropoietin deficiency), haemolytic anaemias, aplastic anaemia, and early iron or B12 deficiency before size changes appear. Normocytic anaemia requires a broader workup.
Macrocytic anaemia (MCV > 100 fL) — red cells larger than normal. The cause is almost always impaired DNA synthesis during precursor cell division. Most common causes: vitamin B12 deficiency and folate deficiency — without these vitamins, cell nuclei cannot divide normally; the cell grows but doesn't divide. Other causes: chronic alcohol use (direct toxic effect on erythropoiesis), hypothyroidism, methotrexate, hydroxyurea, some antiretroviral medications.
An important nuance: when iron deficiency and B12 deficiency coexist, MCV may remain normal — the "double deficiency" masks size changes. Always look at additional red cell indices: MCH, MCHC, and RDW, not MCV alone.
Elevated MCV Without Anaemia: What It Means
MCV can be elevated with normal haemoglobin — and this is also diagnostically significant.
Chronic alcohol use is the classic cause of isolated macrocytosis without anaemia. Ethanol directly disrupts red cell maturation. The effect persists for weeks after stopping alcohol — making MCV a useful indirect marker of chronic use, alongside GGT.
Hypothyroidism slows everything, including erythropoiesis — red cells "over-mature" and enlarge. Unexplained macrocytosis warrants TSH testing.
Pregnancy — mild physiological macrocytosis is normal.
Medications: hydroxyurea, methotrexate, zidovudine — they impair DNA synthesis and predictably cause macrocytosis.
Reticulocytosis — during active recovery after blood loss or haemolysis, large immature reticulocytes appear in circulation, transiently raising MCV.
Low MCV Without Anaemia
Isolated low MCV with normal haemoglobin most often indicates thalassaemia trait — carriage of a defective globin gene. Red cells are small and numerous, and haemoglobin is compensated within normal range. Diagnosed by haemoglobin electrophoresis.
How to Prepare for the Test
MCV is measured within a complete blood count — no separate test exists. Standard preparation: fasting for eight hours, avoid intense activity beforehand. Important: MCV does not change rapidly — it reflects the average age of circulating red cells (which live for 120 days). Acute events (bleeding, onset of deficiency) alter MCV over weeks, not immediately.
When evaluating anaemia, MCV is always interpreted alongside MCH (mean corpuscular haemoglobin), MCHC (mean corpuscular haemoglobin concentration), and RDW (red cell distribution width) — all present in a standard complete blood count with full indices.
When to See a Doctor
Schedule a routine GP appointment if:
- MCV is low and haemoglobin is also low — microcytic anaemia requires investigation.
- MCV is above 100 fL — especially with normal haemoglobin — to exclude B12/folate deficiency or alcohol-related damage.
- MCV is abnormal without an obvious cause (diet, alcohol, medications).
Conclusion
MCV is a navigational marker in anaemia diagnosis: it does not establish a diagnosis on its own, but instantly directs the clinician in the right direction. Small red cells — think iron. Large ones — think B12 and folate. Normal-sized with low haemoglobin — search for other causes. This is why MCV is a mandatory component of every complete blood count.
This article is for informational purposes only. Interpreting test results and prescribing treatment is exclusively the responsibility of a physician.
For informational purposes only
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Please consult a healthcare professional for medical guidance.