Omega-3 Index: Normal Range, Interpretation and How It's Measured
Reviewed by the LabReadAI medical team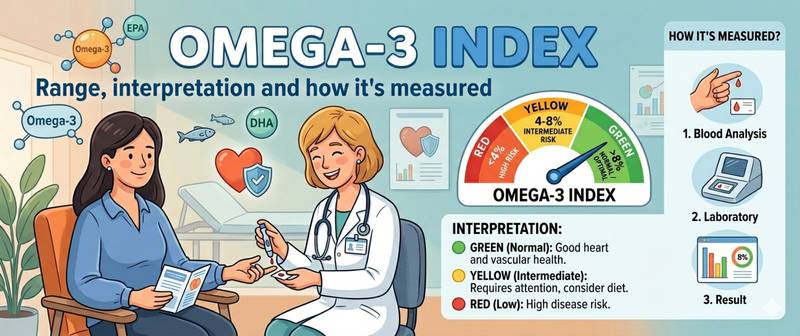
Most people taking fish oil do not know whether it is actually working. The level of omega-3 in the body cannot be assessed by how you feel. The Omega-3 Index solves exactly this problem: it objectively measures how much EPA and DHA is incorporated into red blood cell membranes — an objective marker of omega-3 status throughout the body. Its interpretation is straightforward: the normal Omega-3 Index in most adults is 4–6%, but the target to improve cardiovascular and brain outcomes is 8–12%.
What Is the Omega-3 Index and How Is It Measured?
The Omega-3 Index is the percentage of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) in red blood cell membrane fatty acids.
Formula: Omega-3 Index = (EPA + DHA) / total fatty acids × 100%
Why red blood cells? Their lifespan is 90–120 days, so the fatty acid composition of their membrane reflects mean omega-3 intake over that period — analogous to how HbA1c reflects mean blood glucose over three months.
The assay uses whole blood (not plasma): venous blood is drawn, red blood cells are isolated, and fatty acid profiling is performed by chromatography.
Omega-3 Index Normal Ranges
| Category | Value | Risk |
|---|---|---|
| Deficient | < 4% | High cardiovascular risk |
| Low | 4–6% | Elevated risk |
| Target | 8–12% | Optimal protection |
| Excess | > 12% | No proven harm, rare |
Most Western adults fall in the 4–6% range. The target of 8% was established by researcher William Harris, who developed the Omega-3 Index concept. Below 4% is the high-risk zone, particularly for cardiac outcomes.
Omega-3 and Heart Health
The omega-3 — cardiovascular disease relationship is among the most studied in nutritional science.
Anti-arrhythmic effect. DHA stabilises the electrical conductance of cardiomyocytes. The REDUCE-IT trial (2018) showed that 4 g of EPA daily reduced major cardiovascular events by 25% in patients with hypertriglyceridaemia. Cohort data show that an index above 8% is associated with a 90% lower risk of sudden cardiac death compared with an index below 4%.
Triglyceride reduction. EPA and DHA lower hepatic triglyceride synthesis and circulating triglyceride levels by 20–30%. This is directly linked to C-reactive protein — the inflammatory marker.
Endothelial effects. Omega-3 fatty acids improve vascular wall elasticity, reduce platelet adhesion and lower inflammatory cytokines.
Omega-3, the Brain and Cognitive Function
DHA is the principal structural component of neuronal membranes. The adult brain contains about 20 g of DHA; grey matter is 15–20% DHA by mass.
DHA deficiency is associated with memory impairment, depression and increased Alzheimer's disease risk. Prospective studies show that individuals with a high Omega-3 Index have larger hippocampal volumes and slower age-related cognitive decline.
EPA influences neuroinflammation by suppressing arachidonic acid synthesis and reducing central nervous system inflammation. For those tracking biological age markers, the Omega-3 Index is an essential component — see omega-3 index and longevity.
Why Omega-3 Supplements May Not Work
Not all fish oil forms are equally bioavailable.
Form matters. The triglyceride form (natural fish oil) is absorbed approximately 70% better than ethyl esters (most cheap capsules). The phospholipid form (krill oil) has the highest bioavailability but lower EPA+DHA content by weight.
Fat co-ingestion is essential. Omega-3 fatty acids are fat-soluble. Taking them on an empty stomach reduces bioavailability two to threefold. Always take with a meal containing fat.
Dose. Raising the index to 8% requires approximately 2–3 g of EPA+DHA daily (not grams of fish oil — check the label for EPA+DHA specifically). A standard "1000 mg fish oil capsule" contains only about 300 mg of EPA+DHA — seven to ten times less than needed.
Oxidation. Fish oil oxidises on contact with oxygen. Rancid oil is not only ineffective but potentially harmful. A reliable marker: fish burps immediately after taking the capsule indicate oxidation. Quality oil is odourless and tasteless.
How to Get an Omega-3 Index Test and Improve Your Level
The test requires whole blood drawn from a vein; no special fasting preparation is needed. Re-test after 3–4 months of changing dose or form: this is how long it takes for the erythrocyte pool to fully turn over, giving an accurate reflection of the intervention.
A comprehensive nutritional status assessment also includes vitamin D and C-reactive protein — together these three provide a picture of anti-inflammatory capacity. See the vitamin panel for a full nutritional screen.
For informational purposes only
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Please consult a healthcare professional for medical guidance.