Reticulocytes in Blood: Normal Levels, Causes and Meaning
Reviewed by the LabReadAI medical team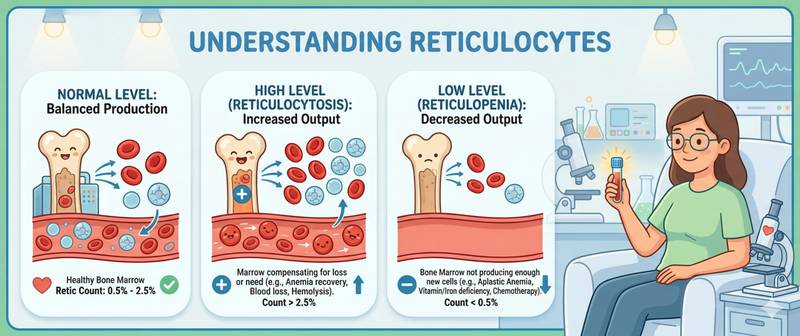
Reticulocytes are young red blood cells that have just left the bone marrow. Their count in blood is a direct window into hematopoietic activity: when reticulocytes rise, the bone marrow is working harder; when they fall, erythropoiesis is suppressed. This is why reticulocytes are indispensable in the differential diagnosis of anemia — they immediately answer the question of whether the bone marrow is the problem or whether the cause lies elsewhere. This marker is rarely included in a routine blood count, but when hemoglobin deviates from normal, it becomes one of the most informative values available.
What Reticulocytes Are and How They Form
Reticulocytes are immature red blood cells — an intermediate stage between the normoblast (a nucleated precursor) and the mature erythrocyte. They form in the bone marrow during erythropoiesis: once an erythroblast expels its nucleus, it enters the bloodstream as a reticulocyte still containing remnants of ribosomes and mitochondria. These organelles, staining with special dyes, produce the characteristic "net-like" pattern — hence the name.
Under normal conditions, a reticulocyte matures in the bloodstream within 1–2 days, becoming a fully mature anucleate red cell. Their proportion in blood directly reflects the rate of new red cell production. The principal driver of erythropoiesis is erythropoietin (EPO), produced by the kidneys in response to tissue hypoxia.
The speed of the reticulocyte response to a stimulus is one of its key diagnostic features. In acute blood loss or hemolysis, the bone marrow sharply increases output: the reticulocytosis peak occurs at 5–7 days. When treatment for iron deficiency anemia begins, reticulocytes start rising within 3–5 days — the first laboratory sign of a therapeutic response.
Normal Reticulocyte Levels
Reticulocytes are expressed in two ways: as a percentage of total red blood cells (relative value) and as an absolute count (cells per liter). The absolute count is more informative in anemia: when total red cell count drops sharply, the relative percentage can appear "normal" even though the bone marrow is actually working inadequately.
| Group | Normal (%) | Normal (×10⁹/L) |
|---|---|---|
| Newborns (days 1–7) | 2.0–6.0 | 110–450 |
| Infants under 2 weeks | 0.5–1.5 | 30–100 |
| Infants 2 weeks – 1 year | 0.5–1.5 | 25–85 |
| Children 1–6 years | 0.5–1.5 | 25–75 |
| Children 6–12 years | 0.5–1.5 | 25–70 |
| Adult men | 0.5–1.5 | 25–75 |
| Adult women | 0.5–2.0 | 25–85 |
| Pregnant women | up to 2.5 | up to 100 |
A more precise tool is the reticulocyte production index (RPI): it corrects the relative percentage for the degree of anemia and the reticulocyte maturation time. RPI = (Reticulocyte% × Patient hematocrit) / (Normal hematocrit × Maturation time). RPI > 2 = adequate bone marrow response; RPI < 2 = inadequate, hypoproliferative anemia.
How to Prepare for a Reticulocyte Test
Reticulocytes are measured as part of an extended complete blood count — using automated hematology analyzers or manual stained smear counting.
- Blood is drawn from a vein in the morning, fasting or 3–4 hours after a light meal — food intake does not significantly affect the result
- Intense exercise the day before transiently raises reticulocytes — avoid strenuous training for 24 hours before the draw
- Blood transfusions in the preceding 4–6 weeks distort the result — donor cells alter the ratio
- Recently initiated treatment with iron, vitamin B12, or folate causes reticulocytosis — this is an expected therapeutic response, not pathology; inform the physician interpreting the result
- For serial monitoring (e.g., tracking treatment response) use the same laboratory each time
Reticulocytes should always be interpreted alongside hemoglobin, hematocrit, and other blood indices — in isolation they provide very limited information.
Causes of High Reticulocytes (Reticulocytosis)
Reticulocytosis — above 2% or > 100×10⁹/L — means the bone marrow has sharply accelerated red cell production. This is always a response to something: blood loss, hemolysis, or the start of anemia treatment.
Blood loss. Acute or chronic blood loss is the most common cause of reticulocytosis. The hypoxia that develops with anemia stimulates EPO production, which drives the bone marrow. The response peaks on days 5–7 after the bleeding episode.
Hemolytic anemia. When red cells are destroyed prematurely — by autoimmune, mechanical, or toxic mechanisms — the bone marrow increases output to compensate. Reticulocytosis in hemolysis is often marked: > 5%, in severe cases > 10–15%. Characteristic combination: reticulocytosis + elevated indirect bilirubin + reduced haptoglobin.
Response to anemia treatment. Three to five days after starting iron therapy for iron deficiency anemia, or vitamin B12/folate for megaloblastic anemia, reticulocytes begin rising — the "reticulocyte crisis." This is the first laboratory sign of an effective treatment response. The peak occurs on days 7–10.
Physiological causes: in newborns during the first week of life, reticulocytosis up to 6% is normal — fetal hemoglobin is being replaced. Moderate reticulocytosis up to 2–2.5% is also physiological in pregnancy. High-altitude residence sustains chronically elevated levels through persistent mild hypoxia.
Less common causes: polycythemia vera — autonomous red cell overproduction; bone marrow metastases displacing normal cells (leukoerythroblastic reaction); extramedullary hematopoiesis in myelofibrosis.
Causes of Low Reticulocytes (Reticulocytopenia)
Reticulocytopenia — below 0.5% or < 20×10⁹/L in the setting of anemia — signals that the bone marrow is failing to keep up. This is a hypoproliferative anemia: the problem is not loss or destruction of red cells, but insufficient production.
Deficiency anemias before treatment. In iron deficiency anemia and megaloblastic anemia (B12 or folate deficiency), the bone marrow cannot produce red cells normally because the necessary substrate is absent — reticulocytes are reduced or at the low end of normal.
Aplastic anemia. Severe damage to bone marrow stem cells — autoimmune, toxic, or idiopathic. Pancytopenia with reticulocytopenia is the classic presentation: simultaneous drops in hemoglobin, leukocytes, and platelets with no reticulocyte response.
Chronic kidney disease. Renal erythropoietin is the primary bone marrow stimulus. When kidney function declines, EPO production falls disproportionately — producing a normochromic normocytic anemia with an inappropriately low reticulocyte count for the degree of anemia.
Malignancy and chemotherapy. Bone marrow infiltration by tumor cells or suppression of hematopoiesis by cytotoxic agents — direct causes of reticulocytopenia.
Other causes: hypothyroidism (reduced metabolic demands decrease erythropoiesis), chronic inflammation (anemia of chronic disease — reticulocytes low or normal despite low hemoglobin), direct alcohol toxicity to erythroblasts.
Reticulocytes in the Differential Diagnosis of Anemia
The main clinical value of reticulocytes is separating anemias into regenerative and aregenerative. This is the first and most fundamental step in diagnosing any anemia.
| Type of anemia | Reticulocytes | Hemoglobin | Typical cause |
|---|---|---|---|
| Hemolytic | Markedly ↑ (> 5%) | Low | Autoimmune hemolysis, hemoglobinopathies |
| Post-hemorrhagic (acute) | ↑ (peak days 5–7) | Low | Bleeding |
| Iron deficiency | Low or normal | Low | Iron deficit: low ferritin |
| Megaloblastic (B12/folate) | Low | Low | Vitamin B12 or folate deficiency |
| Aplastic | Markedly ↓ | Low | Bone marrow failure |
| Renal (EPO deficiency) | Low | Low | CKD, normocytosis |
| Anemia of chronic disease | Low or normal | Low | Inflammation, iron redistribution |
The algorithm is straightforward: in any anemia, look at reticulocytes first. High → investigate blood loss or hemolysis. Low → assess bone marrow, iron stores, B12, folate, kidney function. This two-step approach saves time and avoids unnecessary testing.
When Reticulocyte Abnormalities Require Medical Attention
An isolated minor reticulocyte deviation with normal hemoglobin is generally not a cause for concern. Clinical significance arises when reticulocytes deviate in the context of anemia or progressive symptoms.
Scheduled visit to a doctor when:
- Anemia with below-normal reticulocytes — to identify the cause of hypoproliferation
- Reticulocytosis without an obvious cause (no recent blood loss, no anemia treatment) — rule out hemolysis
- Reticulocytes > 5% combined with jaundice or dark urine
Seek urgent care when:
- Reticulocytopenia combined with pancytopenia — possible aplastic anemia
- Worsening anemia with reticulocytes < 0.2% — critically suppressed bone marrow
- Reticulocytosis > 10% — severe hemolytic crisis
After starting anemia treatment: a follow-up reticulocyte count at 7–10 days confirms the bone marrow response before hemoglobin has time to normalize — this is the earliest reliable marker of treatment efficacy.
This article is for informational purposes only and does not replace professional medical advice. Consult a GP or hematologist if your reticulocyte count is outside the normal range.
For informational purposes only
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Please consult a healthcare professional for medical guidance.