Testosterone After 40 in Men: Normal Levels by Age and Blood Test
Reviewed by the LabReadAI medical team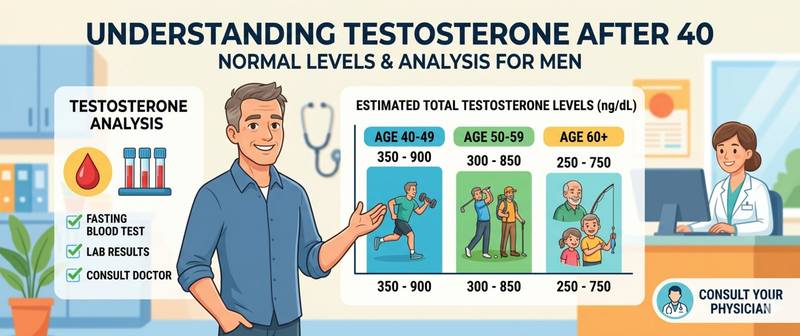
After 30, testosterone in men begins a slow but steady decline — roughly 1–2% per year. By 40, many notice the first signs: less energy, reduced libido, harder to maintain muscle. The question is not whether testosterone will fall, but how fast and whether the drop has crossed a threshold worth acting on. The answer is in a blood test.
How Testosterone Changes After 30 and 40 in Men
Testosterone begins declining around age 30–35 without abrupt drops — gradually, averaging 1–2% per year. By 50, the cumulative decline reaches 15–30% of peak levels; by 65–70, up to 30–50%.
This process is called age-related hypogonadism or andropause. Unlike the female menopause, there is no defined starting point in men — the decline is smooth and individual. Some men maintain high testosterone until 55–60; others develop clinically significant symptoms by 42–45.
What matters is not only the absolute value but the rate of decline. A 20% drop within a single year warrants investigation: behind what looks like "normal aging" there may be a correctable factor — chronic inflammation, vitamin D deficiency, insulin resistance or sleep deprivation.
Normal Testosterone Levels by Age: Reference Table
Reference ranges vary by laboratory and method, but the general age trend is consistent:
| Age | Total testosterone (nmol/L) | Functional optimum (nmol/L) |
|---|---|---|
| 20–30 years | 9.9–27.8 | 18–27 |
| 31–40 years | 8.6–25.3 | 16–25 |
| 41–50 years | 7.6–22.0 | 14–22 |
| 51–60 years | 6.7–19.0 | 12–19 |
| Over 60 | 5.4–17.4 | 10–17 |
The functional optimum is the range in which most men maintain good energy, libido and body composition. Being "within range" and being at the optimum are not the same thing: the lower reference limit (6–8 nmol/L) in a 40-year-old represents a subclinical deficit.
Free Testosterone: Why It Matters More Than Total
Total testosterone is not the full picture. About 60–65% is bound to SHBG (sex hormone-binding globulin) and biologically inactive. Another ~35% is loosely bound to albumin — conditionally active. Only 1–3% circulates as free testosterone and directly acts on target cells.
As men age, SHBG levels rise, further reducing the free fraction — while total testosterone may remain "normal". A man aged 45–50 with total testosterone of 14–15 nmol/L and elevated SHBG may have a genuinely low bioactive fraction and real symptoms.
Normal free testosterone in men: 243–826 pmol/L (70–240 pg/mL), with a marked decline after 50. An alternative measure is the Free Androgen Index (FAI = total testosterone ÷ SHBG × 100); normal for men aged 30–50: 41–137.
Symptoms of Low Testosterone in Men After 40
The symptoms of low testosterone are non-specific and easy to attribute to fatigue, stress or age — which is why hypogonadism often goes undiagnosed for years.
Physical signs: loss of muscle mass and strength despite consistent training; increased visceral fat (especially abdominal); reduced bone density; chronic fatigue unrelated to physical exertion; reduced libido; erectile difficulties.
Cognitive and emotional: reduced concentration and memory; apathy, irritability without obvious cause; disrupted sleep — especially difficulty with morning wake-up.
None of these symptoms is specific to low testosterone. The diagnosis requires both symptoms and laboratory confirmation — the lab result is the anchor.
Testosterone Blood Test for Men: What to Include
Ordering only total testosterone is not enough for proper monitoring after 40. A rational panel includes:
Essential:
- Total testosterone (morning draw, 8–10 am — the daily peak in men)
- SHBG — for calculation of the Free Androgen Index
- LH (luteinising hormone) — to determine whether decline is primary (testicular) or secondary (pituitary)
Extended panel for significant symptoms:
- Free testosterone (direct measurement or calculated by Vermeulen formula)
- Estradiol — in overweight men, testosterone is aromatised to oestrogen at higher rates
- Prolactin — with severe libido loss or gynaecomastia, exclude prolactinoma
The full hormonal monitoring protocol is included in the sex hormone panel. For metabolic context, add a complete blood count, fasting glucose and HbA1c.
Ferritin, Vitamin D and Cortisol: Impact on Testosterone
Testosterone does not operate in isolation — its level depends on several nutritional and hormonal factors that are readily correctable.
Vitamin D. Vitamin D receptors are present in testicular Leydig cells, which are responsible for testosterone synthesis. Vitamin D deficiency (below 50 nmol/L) is associated with a 15–20% reduction in testosterone. Correcting deficiency in deficient men has been shown to raise testosterone by 25–30% in some trials.
Ferritin and chronic inflammation. Chronically elevated ferritin in the context of inflammation suppresses testosterone via the hypothalamic-pituitary-gonadal axis. Pro-inflammatory cytokines directly inhibit LH secretion and reduce cellular testosterone action.
Cortisol — the physiological antagonist of testosterone. Chronic stress and persistently high cortisol suppress GnRH (gonadotropin-releasing hormone), reducing LH and, in turn, testosterone. Overtraining, chronic stress and sleep deprivation lower testosterone precisely through this mechanism.
Optimal Testosterone After 40 vs Lab Reference Range
The laboratory reference range is built on population distribution: the lower limit includes the 2.5% of men with the lowest values. This does not mean that a result at the lower boundary represents good health.
For a man aged 40–50: optimal total testosterone is 15–22 nmol/L; free testosterone should be above 300 pmol/L. At 8–12 nmol/L (lower third of the reference range), most men experience deficiency symptoms even when formally "normal". How to interpret the testosterone result in the context of age, symptoms and trend is detailed in the indicator guide.
When to See a Doctor and Monitoring Plan
Monitoring programme after 40: total testosterone + SHBG once a year, morning draw. If the value drops more than 20% in one year or falls below 12 nmol/L — expand the panel and see a urologist or andrologist.
See a doctor promptly: total testosterone below 8 nmol/L with symptoms; a sharp decline over 6 months without explanation; erectile dysfunction combined with very low LH.
Next steps: before moving to testosterone replacement therapy, correctable factors are worth addressing first — correct vitamin D deficiency, reduce excess weight, improve sleep, lower chronic stress. This alone often raises testosterone by 20–30%. Strategies for raising testosterone — lifestyle and pharmacological — are covered in the guide to how to increase testosterone in men. Testosterone is one of the key hormonal markers of ageing pace — a comprehensive longevity programme is in the article how to live long and healthy. DHEA-S as a marker of adrenal biological age and its relationship with testosterone — DHEA-S and ageing. IGF-1 — the dual anabolic and cancer risk marker — IGF-1 and longevity.
This article is for informational purposes. Interpreting test results and prescribing treatment is the responsibility of a qualified doctor.
For informational purposes only
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Please consult a healthcare professional for medical guidance.