Pregnancy Blood Panel: Tests by Trimester, Norms and Results
Reviewed by the LabReadAI medical team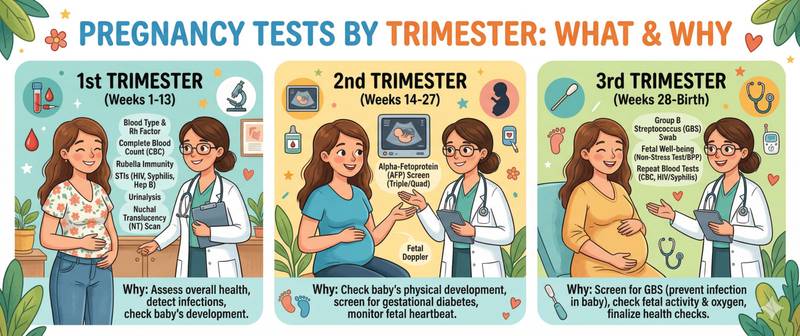
Pregnancy is a period when laboratory monitoring becomes part of caring for two lives at once. The body changes rapidly: normal ranges for many tests differ from non-pregnant values, and some conditions — iron deficiency, thyroid dysfunction, gestational diabetes — develop silently and are only discovered through blood tests. Here is what to test, when, what the results mean, and which abnormalities cannot be ignored.
Why Pregnancy Tests Differ from Standard Reference Ranges
Pregnancy produces physiological changes across every organ system that directly affect laboratory results. By the end of the first trimester, circulating blood volume has increased by 40–50% — almost entirely through plasma expansion. This dilutes red cells and proteins: haemoglobin, albumin, and platelet count all fall physiologically. At the same time, demand for iron, folate, iodine, and vitamin D surges — without supplementation, deficiencies develop quickly.
This is why pregnancy results must be interpreted against pregnancy-specific reference ranges — the standard non-pregnant norms simply do not apply.
First Trimester (Weeks 1–13): Baseline Screening
The first antenatal visit — ideally before weeks 8–10 — establishes the pregnancy diagnosis, identifies baseline deficiencies, and screens for infections that can harm the fetus.
hCG (human chorionic gonadotropin) — confirms pregnancy and tracks its progression. In a healthy early pregnancy, hCG doubles every 48–72 hours through weeks 8–10. Slow rise suggests possible ectopic pregnancy or threatened miscarriage. After weeks 11–12, a physiological decline begins — this is normal.
Haemoglobin and complete blood count — anaemia screening. Physiological thresholds in pregnancy: haemoglobin ≥ 110 g/L in the first and third trimesters, ≥ 105 g/L in the second. Values below these indicate pregnancy anaemia requiring treatment.
Ferritin — iron stores. Falls before haemoglobin does: a level below 30 µg/L indicates depleted stores. Iron deficiency in pregnancy is the leading cause of anaemia and a common contributor to the fatigue often dismissed as "morning sickness."
TSH (thyroid-stimulating hormone) — thyroid function. First-trimester norms are stricter than outside pregnancy: the target is < 2.5 mIU/L. Untreated hypothyroidism during pregnancy impairs fetal neurological development and raises the risk of preterm birth.
Fasting glucose — baseline diabetes screening. A value ≥ 5.1 mmol/L at the first visit meets the WHO 2013 criterion for gestational diabetes without further testing. Values between 5.1–6.9 mmol/L establish the diagnosis on a single measurement.
Vitamin D — deficiency is found in most pregnant women in countries with limited sun exposure. A level below 50 nmol/L requires correction: vitamin D is essential for fetal bone development, immune function, and reducing the risk of pre-eclampsia.
Folate — critical in the first 12 weeks: deficiency during neural tube closure (days 21–28 after conception) dramatically raises the risk of fetal structural defects. Folic acid supplementation ideally begins three months before conception and continues throughout the first trimester.
Blood group and Rh factor — when the mother is Rh-negative and the father Rh-positive, the risk of Rh sensitisation is assessed. Anti-D immunoglobulin is given prophylactically at week 28 and after delivery.
Infection screening: antibodies to HIV, syphilis, hepatitis B (HBsAg) and hepatitis C — mandatory at the first visit and repeated in the third trimester.
Urinalysis — detects urinary tract infections (asymptomatic bacteriuria in pregnancy must be treated) and proteinuria as an early sign of pre-eclampsia.
Second Trimester (Weeks 14–27): Gestational Diabetes and Anaemia Screening
Oral glucose tolerance test (OGTT) — 75 g glucose — the standard gestational diabetes screen at weeks 24–28, offered to all pregnant women whose fasting glucose in the first trimester was < 5.1 mmol/L. Diagnostic thresholds: fasting ≥ 5.1 mmol/L, at 1 hour ≥ 10.0 mmol/L, at 2 hours ≥ 8.5 mmol/L.
Repeat complete blood count — monitoring haemoglobin and platelets. Physiological blood dilution is maximal in the second trimester, so haemoglobin often reaches its lowest values at this point.
Calcium and magnesium — when symptoms are present: leg cramps, pulling pains, irritability. Hypomagnesaemia in pregnancy is a frequent and correctable cause of calf muscle cramps.
Third Trimester (Weeks 28–40): Preparing for Delivery
Repeat infection screening (HIV, syphilis, HBsAg) — at weeks 28–30 and 36.
Coagulation panel — clotting system assessment before delivery. Pregnancy physiologically increases coagulability, raising thrombosis risk. Critical changes may indicate pre-eclampsia or HELLP syndrome.
Repeat complete blood count — the final pre-delivery anaemia screen. Correcting iron deficiency at this stage is particularly important: blood loss in labour is far more dangerous in a woman with an already reduced haemoglobin.
Group B Streptococcus (GBS) — vaginal swab culture at weeks 35–37. If carriage is detected, intrapartum antibiotic prophylaxis is given.
Normal Ranges for Key Pregnancy Tests
| Test | First trimester | Second trimester | Third trimester |
|---|---|---|---|
| Haemoglobin (g/L) | ≥ 110 | ≥ 105 | ≥ 110 |
| Ferritin (µg/L) | > 30 | > 20 | > 15 |
| TSH (mIU/L) | < 2.5 | < 3.0 | < 3.5 |
| Fasting glucose (mmol/L) | < 5.1 | < 5.1 | < 5.1 |
| Vitamin D (nmol/L) | > 50 | > 50 | > 50 |
Reference intervals may vary slightly between laboratories — always compare your result against the range on your own report.
Warning Results: When to Contact Your Doctor Immediately
Contact your obstetrician immediately if: haemoglobin falls below 90 g/L — severe anaemia requiring urgent correction; fasting glucose exceeds 7.0 mmol/L — possible overt diabetes; TSH is below 0.1 or above 10 mIU/L — significant thyroid dysfunction; urine protein exceeds 0.3 g per 24 hours combined with elevated blood pressure — signs of pre-eclampsia; significant coagulation abnormalities appear alongside symptoms.
This article is for informational purposes only. Test ordering, result interpretation and treatment are the responsibility of a qualified obstetrician-gynaecologist.
For informational purposes only
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Please consult a healthcare professional for medical guidance.